

 Dr. Maroon received an athletic scholarship to Indiana University in Bloomington, Indiana where as an undergraduate, he was named a Scholastic All-American in football. Dr. Maroon has successfully maintained his personal athletic interests through participation in 9 marathons and more than 72 Olympic-distance triathlon events. However, his greatest athletic accomplishment is his participation in 8 Ironman triathlons (Hawaii – 1993, 2003, 2008, 2010, 2013; Canada – 1995; New Zealand – 1997; Germany – 2000), where he usually finishes in the top 10 of his age group. Recently, in July 2012 and 2013, he finished second and third, respectively, in his age group in the Muncie, Indiana half Ironman triathlon. In October 2013 he completed his 5th World Championship Ironman in Kona, Hawaii.
Dr. Maroon received an athletic scholarship to Indiana University in Bloomington, Indiana where as an undergraduate, he was named a Scholastic All-American in football. Dr. Maroon has successfully maintained his personal athletic interests through participation in 9 marathons and more than 72 Olympic-distance triathlon events. However, his greatest athletic accomplishment is his participation in 8 Ironman triathlons (Hawaii – 1993, 2003, 2008, 2010, 2013; Canada – 1995; New Zealand – 1997; Germany – 2000), where he usually finishes in the top 10 of his age group. Recently, in July 2012 and 2013, he finished second and third, respectively, in his age group in the Muncie, Indiana half Ironman triathlon. In October 2013 he completed his 5th World Championship Ironman in Kona, Hawaii.The skull base & cranial nerves
The skull base
What is the skull base and skull base region?
When you think of the “skull”, you most likely envision the outside of the skull, as seen on many skeleton pictures. You may not be aware that the skull is not just hollow on the inside – but that there are bone structures inside the skull as well. These bone structures make up the skull base. The skull base provides the base on which the brain rests inside the skull. The skull base region describes the area of and directly around this bony structure. Contained within the skull base region are the eye orbits, ear canals, two carotid arteries, two vertebral arteries, 12 cranial nerves and the blood drainage system of the brain. These many intricate structures make the skull base one of the most complex areas on which to operate.
Recent advances in skull base surgery
Two kinds of disorders or lesions may make skull-base surgery necessary: benign or malignant tumors, and vascular lesions, such as aneurysms, malformations of the veins and arteries, and fistulas (an abnormal connection between vessels).
Traditionally, many lesions at the base of the skull have been inoperable. Surgical techniques simply were not satisfactory, and many patients faced a high risk of neurological problems after surgery. Great advances in diagnostic imaging, surgical techniques and instruments, and a better understanding of the skull-base anatomy have allowed neurosurgeons to remove tumors at the base of the skull. Previously inoperable lesions now can be removed and many surgeries carry far fewer risks to the patient than they used to.
Furthermore, identifying lesions has become less difficult during the past few years thanks to the advent diagnostic tools such as of Magnetic Resonance Imaging (MRI) and angiography. Early detection allows the surgeon to operate sooner, which can help prevent complications. Because most tumors of the skull base are benign when they develop, but can turn malignant over time, early treatment is crucial for the best prognosis, and to maintain optimal function of nerves and arteries in this area.
Reaching the skull base for surgery
Skull-base surgery involves operating within one of three regions of the skull: the anterior, middle or posterior fossa. Neurosurgeons who work within these areas must approach each in a very specific way with regard to the size and type of lesion to be removed. Because of the delicate nature of this type of surgery, patients may be in the operating suite from six to as many as 15 hours or more.
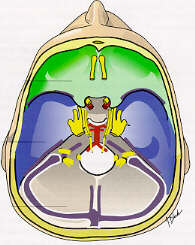 The anterior fossa (green section on drawing)
The anterior fossa (green section on drawing)
The most common type of tumor found in this region of the skull base are meningiomas. Meningiomas are so called because they grow from the meninges, the membranes around the brain and spinal cord. This benign tumor commonly extends through the skull-base bone and down into the bones of the face. Other common problems we see in this area are aneurysms and pituitary and olfactory tumors. To reach such tumors, the neurosurgeon may be required to gently retract the brain from the skull base, allowing removal of the tumor and nearby bone. However, recent advances in the Endoscopic Endonasal Approach (EEA) to access this area of the skull makes less invasive surgery possible. On occasion, surgeons must use transorbital (through the eye socket) or transfrontal (through the face) routes to expose and remove the tumors.
The middle fossa (blue section on drawing)
The middle fossa of the brain may be approached through the side of the skull (transtemporally, subtemporally or pterionally), through the face (transfrontally), or through the nose (transsphenoidally). The surgical team often will include both a neurosurgeon and otolaryngologist to operate within the complicated anatomy of this region of the skull base.
The cavernous sinus is a special part in the middle fossa, located at the border of the anterior fossa. The cavernous sinus houses the carotid artery and multiple cranial nerves. In this small but extremely complex region, it used to be virtually impossible to remove lesions. Largely due to advanced surgical techniques, specific anatomic knowledge and specialized instrumentation, successful surgery within the cavernous sinus is now possible.
The posterior fossa (gray section on drawing)
Neurosurgeons often reach lesions in this area of the skull base through the mastoid region and/or labyrinth of the ear. As such, the base of the skull and posterior fossa are clearly exposed to aid in removing lesions within this area. The posterior fossa also may be approached transorally (through the roof of the mouth) to gain access to the skull base.
Why Dr. Maroon at UPMC?
Lesions of the skull base present a unique challenge to neurosurgeons. In fact, there are very few neurosurgeons in the world who are specially trained and qualified to perform such intricate surgery in the small recesses of the brain. Dr. Maroon is part of this minority of qualified and experienced surgeons. Our neurosurgeons and staff at UPMC also have experience in cerebrovascular surgery (i.e. of the blood vessels in the brain) and perform vascular skull base surgeries. These may involve management of complex vascular and neoplastic (cancer) lesions of the skull base. UPMC provides state-of-the-art instruments and technology to allow the neurosurgeons to obtain optimal results. Furthermore, UPMC Presbyterian Hospital maintains a 24-hour emergency service for stroke, as well as emergency aeromedical transportation.
Cranial nerves – what are they and why are they so important?
There are 12 pairs of cranial nerves, all emerging from the base of the skull and the brain stem. Each pair of nerves is responsible for a specific, basic function such as hearing, smelling, swallowing, blinking, or focusing the eyes. One of each pair of cranial nerves provides feeling and function, or innervates, the right side of the body and the other nerve in the pair innervates the left side.
Tumors of the skull base often affect the cranial nerves, both by their presence and by the steps the surgeon must take to remove the tumor. The result may be a temporary or permanent loss of function of one or more of the cranial nerves. Risk of damage to the cranial nerves depends on the type and location of the tumor.
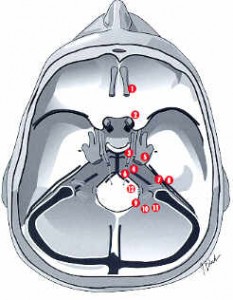
Summary of the function of each Cranial Nerve:
- 1st Cranial Nerve (olfactory nerve) – Responsible for smell. If injured by tumor or surgery for tumor removal, food taste is also altered.
- 2nd Cranial Nerve (optic nerve) – Responsible for vision. A partial injury to this nerve may result is a “field cut” or partial vision loss.
- 3rd, 4th, and 6th Cranial Nerves (oculomotor, trochlear, and abducens) – Controlling movement of the eyeball. Injury can cause double vision. The third cranial nerve also controls pupil dilation.
- 5th Cranial Nerve (trigeminal nerve) – Controls both function and sensation of the face. An injury can result in difficulty chewing and diminished facial sensation or facial numbness.
- 7th Cranial Nerve (facial nerve) – Controls facial movements. An injury can result in a facial “droop”.
- 8th Cranial Nerve (auditory or acoustic nerve) – Responsible for hearing. Skull-base surgery can sometimes leave hearing intact once a tumor on this nerve is removed.
- 9th Cranial Nerve (glossopharyngeal) – Responsible for sensation to the back of the throat.
- 10th Cranial Nerve (vagus nerve) – Protects against choking, and allows for normal swallowing and speech.
- 11th Cranial Nerve (spinal accessory nerve) – Responsible for shrugging shoulders.
- 12th Cranial Nerve (hypoglossal nerve) – Responsible for tongue movement.
Tri-State Neurosurgical Associates-UPMC
Administrative Oakland Office Address:
Presbyterian University Hospital
Department of Neurosurgery
Suite 5C
200 Lothrop Street
Pittsburgh, PA 15213
Phone: 1-888-234-4357
© 2013 Tri-State Neurosurgical Associates – UPMC