

 Dr. Maroon received an athletic scholarship to Indiana University in Bloomington, Indiana where as an undergraduate, he was named a Scholastic All-American in football. Dr. Maroon has successfully maintained his personal athletic interests through participation in 9 marathons and more than 72 Olympic-distance triathlon events. However, his greatest athletic accomplishment is his participation in 8 Ironman triathlons (Hawaii – 1993, 2003, 2008, 2010, 2013; Canada – 1995; New Zealand – 1997; Germany – 2000), where he usually finishes in the top 10 of his age group. Recently, in July 2012 and 2013, he finished second and third, respectively, in his age group in the Muncie, Indiana half Ironman triathlon. In October 2013 he completed his 5th World Championship Ironman in Kona, Hawaii.
Dr. Maroon received an athletic scholarship to Indiana University in Bloomington, Indiana where as an undergraduate, he was named a Scholastic All-American in football. Dr. Maroon has successfully maintained his personal athletic interests through participation in 9 marathons and more than 72 Olympic-distance triathlon events. However, his greatest athletic accomplishment is his participation in 8 Ironman triathlons (Hawaii – 1993, 2003, 2008, 2010, 2013; Canada – 1995; New Zealand – 1997; Germany – 2000), where he usually finishes in the top 10 of his age group. Recently, in July 2012 and 2013, he finished second and third, respectively, in his age group in the Muncie, Indiana half Ironman triathlon. In October 2013 he completed his 5th World Championship Ironman in Kona, Hawaii.Cranial Anatomy
- Brain Covering
- Cranial Nerves
- Brain Tumors
- Skull Base Surgery
- Pituitary Tumors
The human brain is generally well protected from outside injury. It is firmly surrounded by three layers of membranes, encased in a rigid skull (the cranium), and covered by a muscular scalp. Each of these barriers to the brain is important, because brain tissue is fragile and can be unforgiving if injured.
 The three layers of membranes (the meninges) that cover the brain and the spine are the:
The three layers of membranes (the meninges) that cover the brain and the spine are the:
- Dura mater, a tough and fibrous protective membrane that lines the skull from the inside
- Arachnoid mater, a thin membrane which provides cushioning
- Pia mater, a very fine membrane, and the only one directly lining the surface of the brain by following all the grooves. It provides nourishment to the brain through its many fine blood vessles.
The space between the arachnoid mater and the pia mater is filled with a fluid that provides nutrients as well as shock-absorption to the brain: the cerebrospinal fluid (CSF). The CSF also surrounds the spinal cord and fills open spaces (ventricles) inside the brain. The amount of CSF that circulates around the brain normally stays the same. The CSF helps to maintain a constant pressure inside the skull, known as intracranial pressure (ICP).
Cranial nerves – what are they and why are they so important?
There are 12 pairs of cranial nerves, all emerging from the base of the skull and the brain stem. Each pair of nerves is responsible for a specific, basic function such as hearing, smelling, swallowing, blinking, or focusing the eyes. One of each pair of cranial nerves provides feeling and function, or innervates, the right side of the body and the other nerve in the pair innervates the left side.
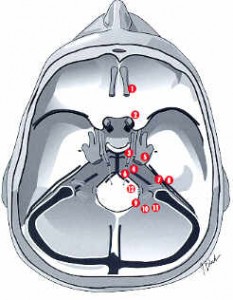 Summary of the function of each Cranial Nerve:
Summary of the function of each Cranial Nerve:
- 1st Cranial Nerve (olfactory nerve) – Responsible for smell. If injured by tumor or surgery for tumor removal, food taste is also altered.
- 2nd Cranial Nerve (optic nerve) – Responsible for vision. A partial injury to this nerve may result is a “field cut” or partial vision loss.
- 3rd, 4th, and 6th Cranial Nerves (oculomotor, trochlear, and abducens) – Controlling movement of the eyeball. Injury can cause double vision. The third cranial nerve also controls pupil dilation.
- 5th Cranial Nerve (trigeminal nerve) – Controls both function and sensation of the face. An injury can result in difficulty chewing and diminished facial sensation or facial numbness.
- 7th Cranial Nerve (facial nerve) – Controls facial movements. An injury can result in a facial “droop”.
- 8th Cranial Nerve (auditory or acoustic nerve) – Responsible for hearing. Skull-base surgery can sometimes leave hearing intact once a tumor on this nerve is removed.
- 9th Cranial Nerve (glossopharyngeal) – Responsible for sensation to the back of the throat.
- 10th Cranial Nerve (vagus nerve) – Protects against choking, and allows for normal swallowing and speech.
- 11th Cranial Nerve (spinal accessory nerve) – Responsible for shrugging shoulders.
- 12th Cranial Nerve (hypoglossal nerve) – Responsible for tongue movement.
Tumors of the skull base often affect the cranial nerves, both by their presence and by the steps the surgeon must take to remove the tumor. The result may be a temporary or permanent loss of function of one or more of the cranial nerves. Risk of damage to the cranial nerves depends on the type and location of the tumor. Dr. Maroon will always discuss your specific situation with you and explain your individual risk.
Disclaimer:
Every effort has been made by the author(s) to provide accurate, up-to-date information. However, the medical knowledge base is dynamic and errors can occur. By using the information contained herein, the viewer willingly assumes all risks in connection with such use. Neither the author nor UPMC shall be held responsible for errors, omissions in information herein nor liable for any special, consequential, or exemplary damages resulting, in whole or in part, from any viewer(s)’ use of or reliance upon, this material.
CLINICAL DISCLAIMER:
Clinical information is provided for educational purposes and not as a medical or professional service. Person(s) who are not medical professionals should have clinical information reviewed and interpreted or applied only by the appropriate health professional(s).
For questions or comments, please contact: Email Dr Maroon
© 2013 Tri-State Neurosurgical Associates – UPMC
Tri-State Neurosurgical Associates-UPMC
Office Addresses:
Administrative Oakland Office
Presbyterian University Hospital
Department of Neurosurgery
Suite 5C
200 Lothrop Street
Pittsburgh, PA 15213
Phone: 1-888-234-4357